Canada stands among the top countries with the highest Out-of-Pocket Expenses for diabetes supplies

News • November 14, 2022
1. Introduction
Without insulin, a person living with type 1 diabetes (T1D) cannot survive. Despite its discoverers’ intent that insulin be accessible to all who need it and their desire to prevent its exploitation by monopolies, it has become a commercial product, grossing huge profits over recent decades. More than 100 years after its discovery, many people with T1D die because they cannot access or afford insulin and other essential diabetes supplies. Others face extreme financial burdens, paying 20-100% or more of their monthly income towards diabetes management. T1International, a non-profit advocating for the rights of people with T1D worldwide, and others have documented countless deaths resulting from insulin rationing, and called for international declarations prioritizing insulin access. Market dominance by three insulin manufacturers, patent evergreening, price discrimination, and supply-chain inefficiencies have been cited as contributors to high prices in the absence of governmental regulation. In many countries, healthcare systems lack or leave gaps in coverage for diabetes treatment, contributing to rationing of insulin and supplies.
Various studies have investigated diabetes-related out-of-pocket expenses (OoPEs) for particular products or focused on insulin rationing associated with cost in one clinic or region. Health Action International found extreme price variation of glargine products across 47 countries. Herkert and colleagues surveyed patients living with T1D from one US clinic and found 26.5% rationed insulin due to costs. Analyzing 2021 National Health Interview Survey data, Gaffney and colleagues estimated insulin rationing prevalence among US adults with T1D to be 18.6%, and Fang and Selvin found 23.6% of individuals with T1D younger than 65 rationed insulin due to cost. T1International aims to add to existing literature through its Out-of-Pocket Expenses (OoPEs) survey, which it has carried out every two years since 2016. To our knowledge, this was the first and remains the largest global survey comparing self-reported expenses and rationing of insulin and diabetes supplies.
Using 2020 OoPEs survey data, Pfiester et al. found people with T1D reporting significant OoPEs and rationing of insulin and other diabetes supplies, and negative impacts from the COVID-19 pandemic on access and affordability of supplies. Through quantitative and qualitative analysis of 2022 OoPEs survey data, the present study investigates i) the status of OoPEs and rationing among people with T1D, ii) factors contributing to OoPEs and rationing, and iii) the current impact of the COVID-19 pandemic on access and affordability of insulin and diabetes supplies among people with T1D.
2. Materials and Methods
2.1 Survey Design and Procedures
An anonymous, web-based, cross-sectional survey was conducted in English from May through September 2022 using the Research Electronic Data Capture (REDCap) tool hosted at Cincinnati Children’s Hospital Medical Center. As previously described, this survey was patient-designed. Updated questions included newer insulins and diabetes supplies, as well as previously omitted categories of expenses. Eight volunteers living with T1D across seven countries pilot tested the survey on various devices and suggested improvements related to formatting and applicability across different country contexts.
The survey introductory text informed individuals that their participation was voluntary, and consent was requested before proceeding to survey questions. Participants were asked to indicate whether they had no coverage for any of their diabetes-related costs, partial coverage, or full coverage, paying nothing out-of-pocket. They reported monthly out-of-pocket expenses (OoPEs) in their currency of choice for the following categories: 1) devices, including insulin pumps and continuous (or flash) glucose monitors (CGM), 2) insulin, 3) pen needles and syringes, and 4) blood glucose testing strips. Participants also reported the price per product paid for a glucagon emergency shot or nasal spray, if applicable. Additionally, they provided free text comments to two open-ended questions. The study was declared low-risk and granted ethical exemption by the Human Research Ethics Committee – Humanities (HREC-HS) of University College Dublin. T1International and its global volunteers advertised the survey on social media.
2.2 Data Analysis
Quantitative analyses were conducted within the R statistical framework. Currencies were converted to USD with the priceR package. The distribution of the monthly OoPEs was investigated, and three outlier respondents with expenses exceeding 5,000 USD per month were removed from further analysis. Per-product expenses for glucagon were analyzed separately from monthly OoPEs.
Open-ended responses were analyzed by two of the authors using template analysis. The researchers familiarized themselves with the data and identified preliminary themes related to the reasons for and impacts of OoPEs and rationing. Through critical dialogue, they created a codebook and independently coded a subset of 34 data observations to assess intercoder reliability. The codebook and definitions were revised after further discussion, and all data were analyzed deductively using the revised codebook. This process iteratively updated the codebook, which ultimately consisted of 18 codes with 15 subcodes and identified six primary themes.
3. Results
3.1 Countries represented and healthcare coverage of participants
A total of 1,122 responses were recorded. Of these, 28 were removed for lacking explicit consent, 21 for being under 18 years old, 54 for omitting currency of choice, 5 for missing country information, 3 due to outlying monthly costs (see section 2.2), and 3 were manually identified as duplicates, leaving a total of 1,008 records representing 69 countries.
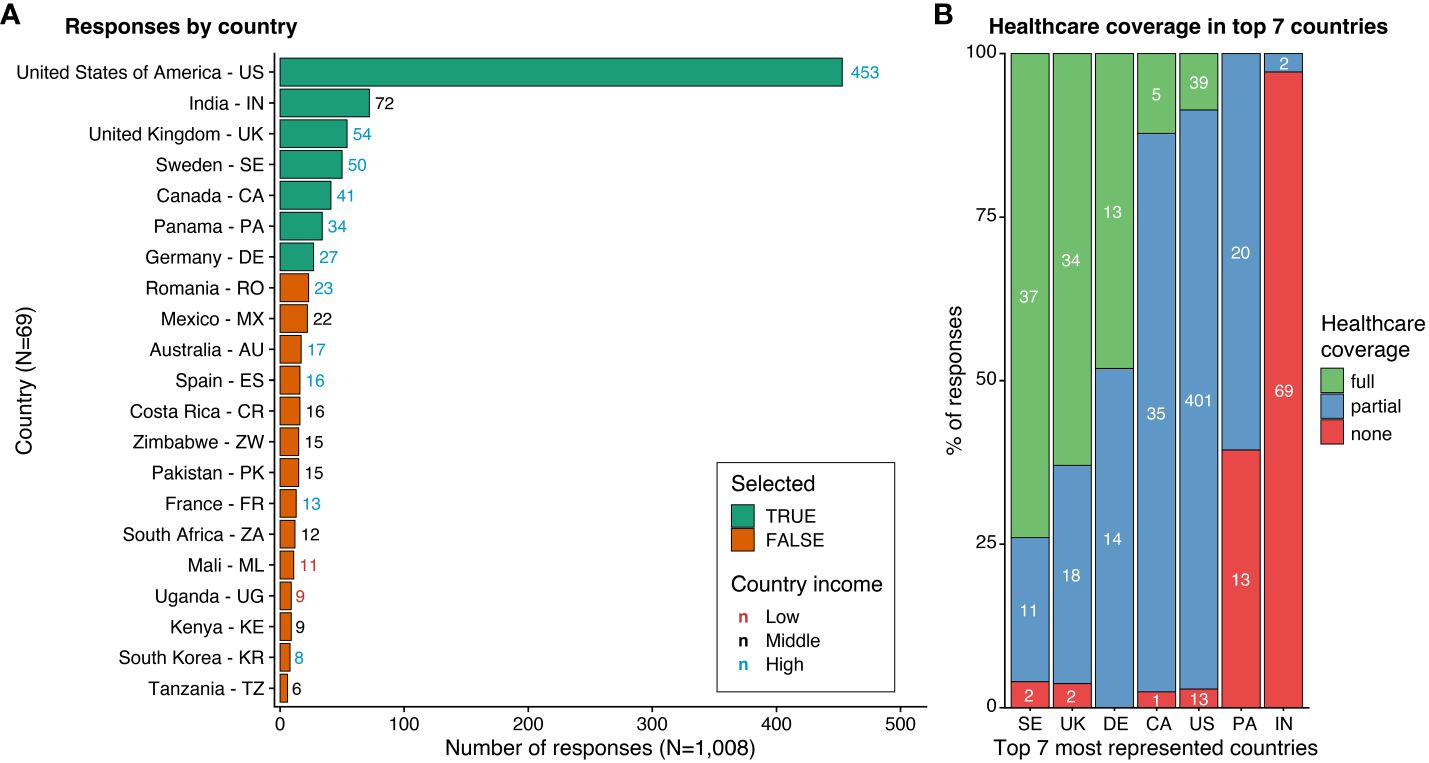
Total Responses by Country and Healthcare Coverage in the Seven Most Represented Countries
(A) The listing of countries (Y-axis) is ordered by the number of responses (X-axis). Countries are indicated by their full name, followed by their alpha-2 code. The seven most represented countries, which were selected for further analysis, are highlighted in green, while the others are shown in orange. Only countries with more than four respondents are included.
(B) The ratio of reported healthcare coverage levels (Y-axis, percentage) is shown for the seven most represented countries (X-axis). Colors indicate the type of healthcare coverage. White numbers denote the number of responses.
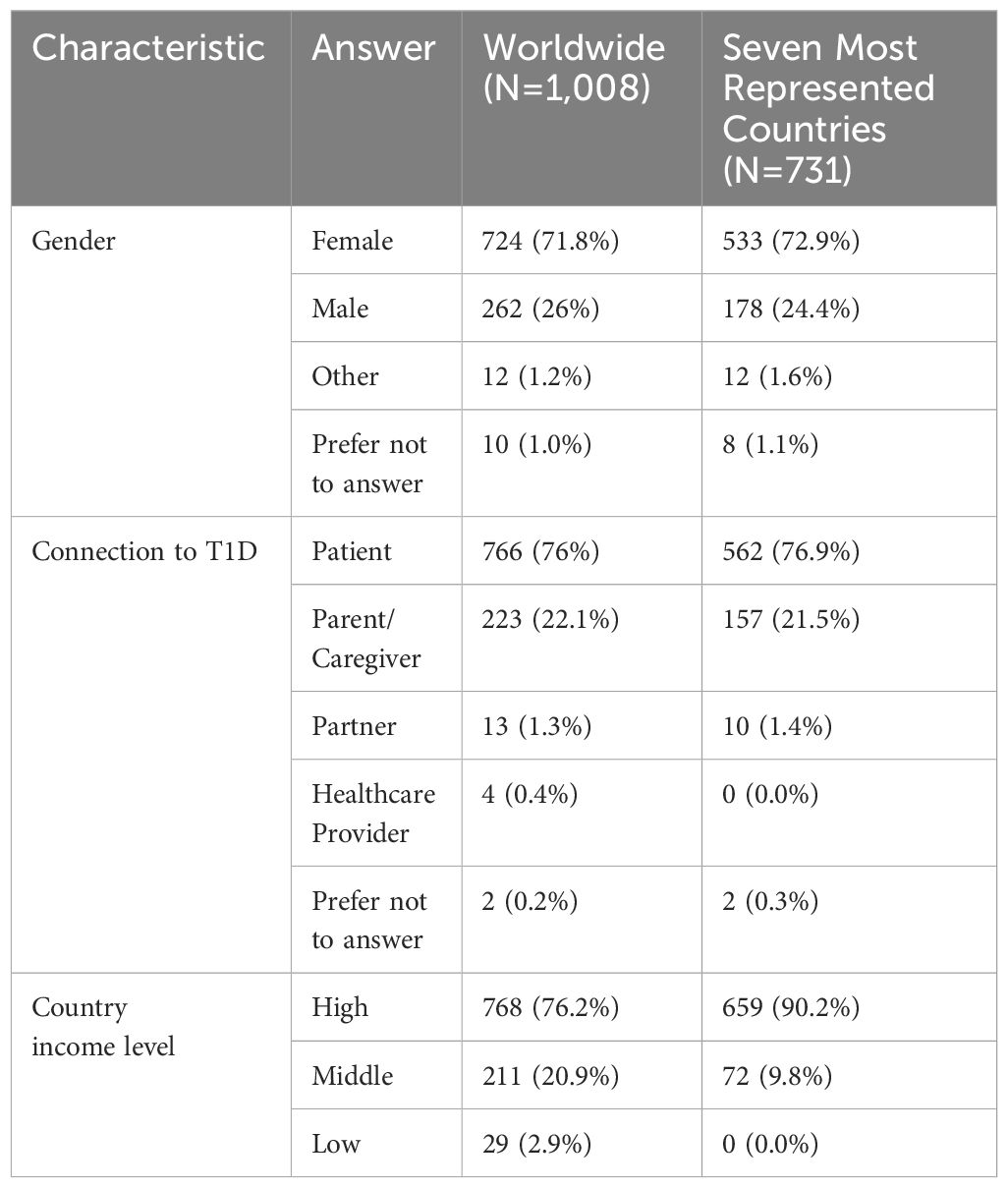
Out of the 1,008 responses included in the analysis, 724 (71.8%) identified as female, 766 (76%) were adults living with T1D, and 223 (22.1%) were parents/caregivers (Table 1). A threshold of 25 responses was used to determine which countries would be included in the comparison sample. This resulted in a total of 731 responses from seven countries: the United States (US), India, the United Kingdom (UK), Sweden, Canada, Panama, and Germany.
The healthcare coverage composition of participants varied across these countries. Sweden had mostly full coverage (74%), followed by the UK (63%). Germany had a mix of full (48.1%) and partial (51.9%) coverage. In contrast, the US (88.5%) and Canada (85.4%) participants reported mostly partial coverage. Panama had mostly partial coverage (60.6%) with the remaining having no coverage (39.4%), while India had mostly no coverage (97.2%).
3.2 OoPEs in the Seven Most Represented Countries
Participants in the seven most represented countries who had partial healthcare coverage reported the highest mean monthly out-of-pocket expenses (OoPEs), averaging 434.9 USD, which was roughly 90 USD higher than those with no healthcare coverage. Participants with full healthcare coverage reported the lowest mean monthly OoPEs, at just 21.2 USD. This amount was over 300 USD less than those with no healthcare coverage and more than 400 USD less than those with partial healthcare coverage.
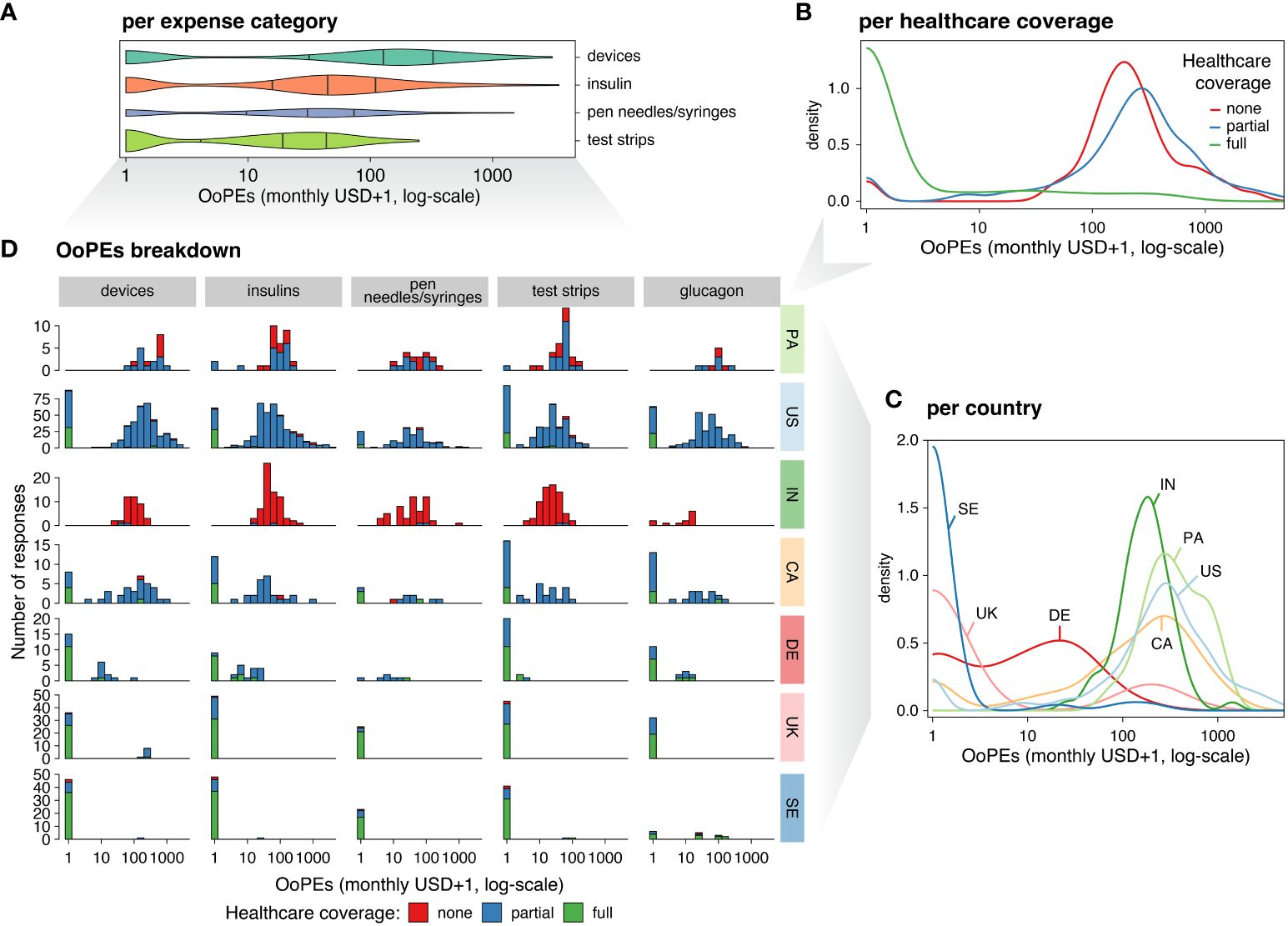
Overview of Out-of-Pocket Expenses (OoPEs) in the Seven Most Represented Countries
(A) Violin plot of self-reported OoPEs (X-axis) indicated in USD (with a pseudocount of +1, log-scale), covering expenses for devices, insulin, pen needles and/or syringes, and testing strips (Y-axis). The strips category (green) includes blood glucose testing strips, while the devices category (teal) covers insulin pumps and CGMs. The insulin category (orange) includes short-acting, long-acting, mixed, and other types of insulin. Violin ticks represent quantiles (25%, 50%, and 75% from left to right, respectively), with the area of the plot proportional to the number of responses.
(B) Density distribution of OoPEs (X-axis, as in A) by healthcare coverage level (colors).
(C) Density distribution of OoPEs (X-axis, structured as in A) by country (colors).
(D) Breakdown of OoPEs (organized as in A) by expense category (columns), country (rows), and healthcare coverage level (bar colors). The Y-axis shows the number of respondents.
The highest mean monthly OoPEs were reported for devices, with the greatest standard deviation (SD) seen in this category. Insulin was the second-highest category for mean monthly OoPEs, with more individuals reporting expenses in this category than any other, regardless of healthcare coverage or country. Monthly OoPEs for pen needles and syringes were higher than for test strips, although they were reported by a smaller percentage of individuals. The mean per-product cost for glucagon was 57.6 USD.
Participants from the US reported the highest mean monthly OoPEs (471.1 USD), followed by Panama, Canada, and India. The lowest mean monthly OoPEs were reported in the UK, Germany, and Sweden. Notably, the SD of OoPEs was highest in the US, 396.4 USD greater than any other country, and the median expenses in Panama were higher than those in the US. Additionally, median OoPEs in Germany were higher than in the UK. Test strip costs were highest in Panama compared to other countries, independent of healthcare coverage level.
Device use was common across all seven countries, with 87.6% of participants reporting CGM use and 63.2% reporting insulin pump use. CGM use was reported by over 90% of participants in Germany, Sweden, Canada, the US, and the UK, while more than 50% of participants in Panama and India also reported CGM use. Insulin pump use was reported by over 70% of participants in the US, over 60% of participants in Germany, Sweden, and Canada, and over 50% of participants in the UK. Additionally, nearly 30% of participants in Panama and nearly 17% of participants in India reported insulin pump use.
3.3 Rationing of Insulin and Glucose Testing Supplies
3.3.1 Worldwide Rationing
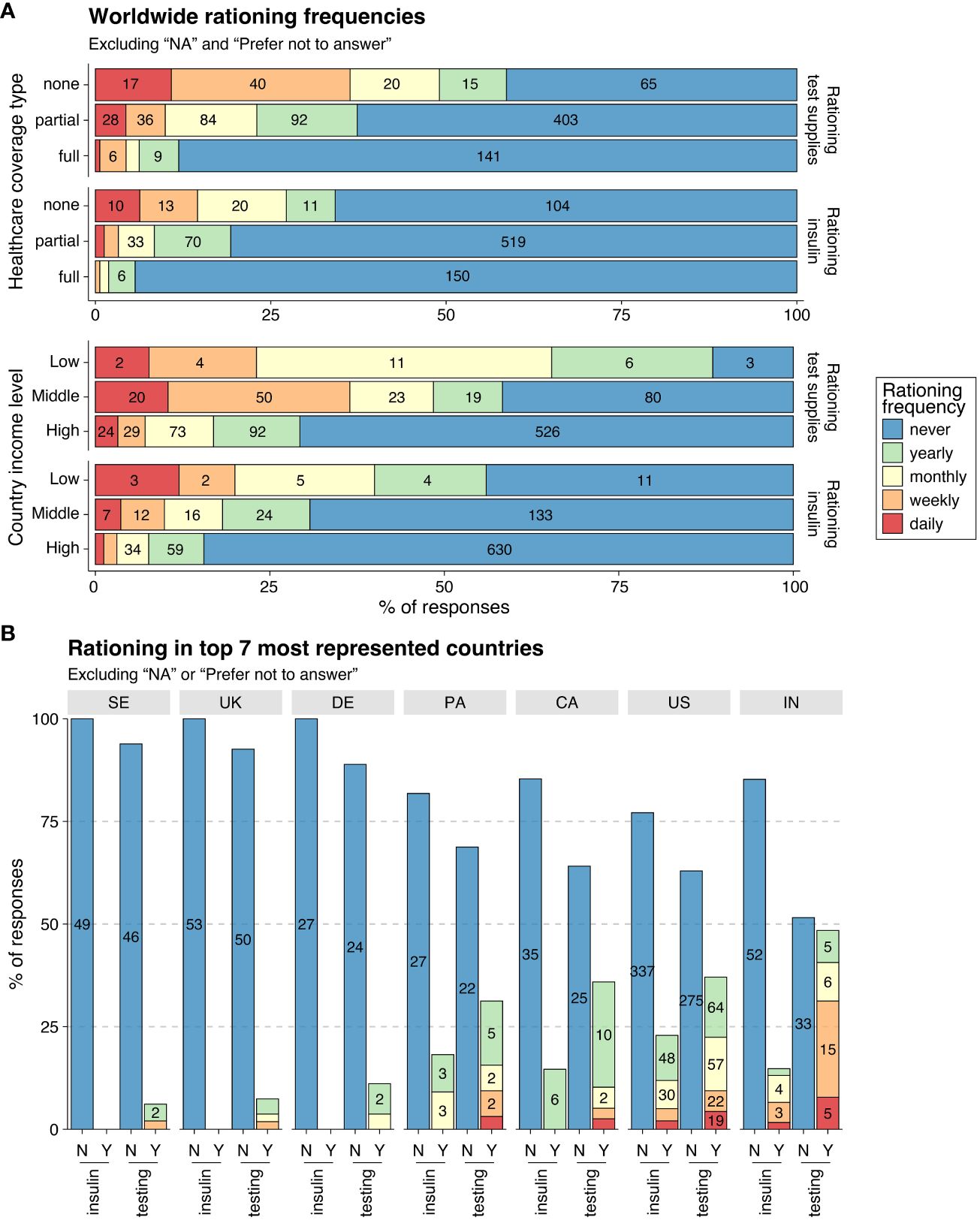
Among all 1,008 participants worldwide, 19.5% rationed insulin and 36.6% rationed glucose testing supplies. Among those living in low-income countries, 56% rationed insulin and 88.5% rationed glucose testing supplies at some point over the past year. There was a visible negative correlation between the level of healthcare coverage and rationing frequency for both testing supplies and insulin. Rationing was most prevalent for individuals with no healthcare coverage, with 34.2% rationing insulin and 58.6% rationing testing supplies at some point over the past year.
3.3.2 Rationing in the Seven Most Represented Countries
Insulin rationing was reported by 21.2% of participants across the US, Panama, India, and Canada, and by no participants in Sweden, the UK, or Germany. The US had the highest percentage of participants rationing insulin at some point over the previous year, followed by Panama, India, and Canada. The frequency of insulin rationing varied across the four countries. No participants from Canada rationed more often than yearly, and no participants from Panama rationed more often than monthly, while participants in the US and India rationed weekly or more.
Overall, rationing of glucose testing supplies was more common than insulin rationing, with 32.3% of participants across the seven countries reporting rationing testing supplies at some point over the past year. However, the prevalence and frequency of rationing varied widely across countries. India had the highest percentage of participants rationing testing supplies at some point, followed by the US, Canada, and Panama. A much smaller percentage of participants rationed testing supplies at some point in Germany, the UK, and Sweden. No participants in Germany rationed more often than monthly, whereas in the UK and Sweden, a small percentage of participants rationed weekly. While rationing glucose testing supplies at some point in the US and Canada was similar, a higher percentage of participants in the US rationed monthly or more often compared to Canada. India had the highest percentage of participants rationing weekly or more.
3.4 Impact of COVID-19 in the Seven Most Represented Countries
Self-reported negative impacts of the COVID-19 pandemic on access and/or affordability of insulin and/or supplies varied across countries. The highest proportion of affected participants were from Panama, with 67.7% reporting challenges. Similarly, participants from the US (58.5%) and India (56.9%) were significantly impacted. In Canada, roughly half of participants reported access and/or affordability challenges from the pandemic, while much smaller percentages of participants from Germany (29.6%), the UK (25.9%), and Sweden (14%) experienced negative impacts.
3.5 Qualitative Analysis Results
Qualitative analysis of responses to open-ended questions identified six primary themes: “Healthcare system improvements needed”; “Problems with insurance and national or state healthcare coverage”; “Strengths of national or state healthcare coverage”; “Other diabetes-related expenses”; “Mental health impacts”; “Limits to life choices”; and “Human Rights.” Below, we detail each theme using participant quotes.
3.5.1 Healthcare System Improvements Needed
Overwhelmingly, participants called on their governments for affordable access to insulin and diabetes supplies, highlighting the potential cost savings:
“Make CGM access available for everyone! It will save you money in healthcare hospital visits for people with T1D.” (Person with T1D, partial healthcare coverage, Canada)
In India, several participants wanted T1D classified as a disability to ensure healthcare coverage for diabetes supplies: “T1D is not covered by health insurance in India. Consider T1D as a disability and support the person.” (Parent/caregiver of a child with T1D, no healthcare coverage, India)
Inaccessibility compounded by unaffordability was a concern for many participants in Panama: “In my region, it is too expensive, or the state-of-the-art products for diabetes do not exist. So, we cannot give our children the best treatment.” (Parent/caregiver of a child with T1D, partial healthcare coverage, Panama)
3.5.2 Limits to Life Choices
Participants reported sacrificing other basic needs due to high diabetes-related OoPEs: “Stop making me choose between buying diabetes supplies and food.” (Person with T1D, partial healthcare coverage, US)
The cost of diabetes management also influenced participants’ broader life choices:
“I also chose which province to live in based on which has the best coverage for diabetes supplies.” (Person with T1D, full healthcare coverage, Canada)
One participant in the US with partial healthcare coverage described how the high costs affected family decisions: “I had to put off trying for another child because my insulin was so expensive. We could not afford another child along with the cost of my diabetes.”
3.5.3 Mental Health Impacts
Participants described the stress and anxiety of being unable to afford or access supplies:
“There is also the emotional cost of the stress of worrying if supplies will last or arrive in time.” (Person with T1D, partial healthcare coverage, US)
“Managing diabetes is both mentally and financially draining.” (Parent/caregiver of a person with T1D, no healthcare coverage, India)
Participants also discussed the varying recognition of the need for mental healthcare:
“Sweden may be one of the few countries in the world that covers nearly all diabetes-related costs. What many of us miss though is more attention to interrelated conditions that make it difficult to get your diabetes under control, such as mental health.” (Person with T1D, full healthcare coverage, Sweden)
3.5.4 Problems with Insurance and National or State Healthcare Coverage
Many participants from the US described insurance as expensive and burdensome: “40% of my monthly paycheck goes towards insurance and I still have copays and out-of-pocket costs.” (Person with T1D, partial healthcare coverage, US)
“Why do I have to plead, negotiate, yell, follow up, and chase down the drugs and supplies I need to stay alive every month?” (Person with T1D, partial healthcare coverage, US)
Others in the US were unable to access insurance:
“We make too much to qualify for any assistance, yet not enough for private insurance. I’m tired of feeling sick because I cannot afford the insulin I should be on or see a doctor.” (Person with T1D, no healthcare coverage, US)
A parent/caregiver of a child with T1D with partial coverage from Panama feared the loss of healthcare coverage as their child became an adult:
“The government covers diabetes supplies only because my child is underage (18 years). Once he is over 18, he will no longer have priority access to these supplies.”
One person living with T1D from Canada, with partial healthcare coverage, spoke to its limits: “I am fortunate to have 80% coverage, but I have to pay upfront and get reimbursed in a week. That week makes a big difference, especially when supplies are only dispensed for 30 days. I know I am one of the lucky ones, but I am still struggling.”
3.5.5 Strengths of National or State Healthcare Coverage
Some participants from countries with universal healthcare described their healthcare coverage positively:
“I am always really appreciative that where I live, there will always be a safety net for my insulin needs through the government. I know I’m incredibly lucky to be a diabetic in Canada and not in another country without public healthcare.” (Person with T1D, full healthcare coverage, Canada)
Others acknowledged that their healthcare is funded by taxes:
“The healthcare system here is socially funded, but the tax (National Insurance) premium that pays for this is 23% of my gross income. The supplies are not free, but they are free at the point of delivery.” (Person with T1D, full healthcare coverage, UK)
In the US, a few participants with full healthcare coverage spoke positively about specific national or state programs:
“My daughter receives California Children’s Services, which covers her for anything diabetes-related. Dexcom is covered as a pharmacy benefit by Medi-Cal, making all these things easily accessible.” (Parent/caregiver of a child with T1D, full healthcare coverage, US)
3.5.6 Other Diabetes-Related Expenses
Participants noted additional diabetes-related costs that were not captured in their reported OoPEs, including hypoglycemia treatment, alcohol swabs, mental healthcare, and specialist visits:
“We have to do quarterly lab tests for my kid to check for the progression and onset of other autoimmune problems. It costs us around 100,000 INR [1,210.47 USD] per year.” (Parent/caregiver of a child with T1D, no healthcare coverage, India)
Some participants spoke about how rationing due to costs led to complications:
“I had to ration my insulin and diabetes supplies when I was uninsured and underinsured. There were insurance plans I had that did not cover insulin pump supplies. My health deteriorated, and now I’m in end-stage renal failure on dialysis.” (Person with T1D, partial healthcare coverage, US)
3.5.7 Human Rights
Many participants used human rights-based language to express their frustration:
“Insulin is a basic human right. I know I’m privileged and have never known the pain of rationing, but I will keep fighting for our right to live as long as it takes.” (Person with T1D, partial healthcare coverage, US)
“It is not a choice. It is literally life or death.” (Person with T1D, partial healthcare coverage, Canada)
Participants also expressed a desire for equity in diabetes care:
“People with diabetes should not be discriminated against by policies that support insulin pumps for specific age groups and not others. And no one with diabetes should ever have to choose between taking their life-saving medication, feeding their families, or paying rent.” (Person with T1D, partial healthcare coverage, Canada)
4. Discussion
This study highlights the significant financial burden that people with T1D face in the absence of full healthcare coverage, which leads to the rationing of insulin and other diabetes supplies. Even in this sample, consisting mostly of participants from high-income countries, a considerable number reported rationing insulin and glucose testing supplies.
Results demonstrated global inequities in out-of-pocket expenses (OoPEs) and subsequent rationing. In the seven most represented countries, OoPEs and rationing were much higher for those with partial or no healthcare coverage compared to those with full healthcare coverage. Participants in Germany, the UK, and Sweden reported low or no OoPEs, no insulin rationing, and lower levels of rationing of testing supplies. In contrast, participants from the US, Panama, Canada, and India reported high monthly OoPEs (over 200 USD) and associated rationing of both insulin and testing supplies. Notably, US participants continued to report insulin rationing rates over 20% and glucose testing supply rationing rates nearing 40%, which aligns with previous studies. In India, a lower-middle-income country, people with T1D do not receive protections under the Rights of Persons with Disabilities Act of 2016, leaving them without assistance for diabetes-related costs. Additionally, Canada’s lack of universal pharmacare contributes to higher costs and rationing of supplies, while in Panama, access to newer insulins is limited and supply shortages are common. The US, one of the wealthiest countries in the world, reported the highest mean monthly OoPEs, highlighting significant inequities in healthcare access.
In our seven-country analysis, participants with no healthcare coverage for diabetes-related expenses reported slightly lower OoPEs than those with partial coverage, likely due to higher levels of rationing among those with no coverage. Partial healthcare coverage, while reducing some costs, often puts advanced diabetes technologies within reach, but still places a significant financial burden on individuals, limiting their choices and leading to higher OoPEs.
The ongoing impact of the COVID-19 pandemic on access and affordability of insulin and supplies remained significant, especially in Panama, the US, and India. However, increased availability of vaccines and therapeutics likely contributed to more stable supply chains compared to earlier in the pandemic.
Rationing of glucose testing supplies was more common than insulin rationing, a finding consistent with previous surveys. The lack of universal guidelines for the recommended frequency of self-monitoring is problematic, particularly in countries like India, where treatment recommendations are often adapted to a patient’s financial limitations.
Our qualitative analysis emphasized the variability in healthcare coverage and access to care, especially in countries without comprehensive universal healthcare systems. Many participants reported conditional coverage or partial access to needed supplies, which placed them at continued risk of rationing. Additionally, participants noted that healthcare systems posed other challenges beyond high OoPEs, such as delayed access to supplies due to discrepancies in prescription practices across provinces or regions.
The study’s strengths include patient involvement in survey design and analysis, and increased representation from countries outside the US. However, limitations such as potential bias due to the English-only, electronic format of the survey, and the relatively advantaged socioeconomic status of participants should be noted.
Future versions of the survey would benefit from translations into multiple languages and wider distribution to ensure representation from non-English speakers and individuals with lower access to care. Further research should explore the broader impacts of rationing, including restrictions on food and other necessities, and the financial burdens faced by people living with T1D.
5. Conclusion
The financial burden of managing type 1 diabetes remains excessively high, leading to the widespread rationing of insulin and diabetes supplies. Rationing continues to affect a significant portion of the global T1D population, with 1 in 5 people in our sample rationing insulin. The study underscores the need for continued advocacy by T1International and other organizations, as well as for healthcare system reforms and global price reductions for insulin and diabetes supplies. Ensuring affordable and equitable access to diabetes care, including advanced technologies, is essential for the health and survival of individuals with T1D.
Data availability statement
The original contributions presented in the study are publicly available. This data can be found on the GitHub repository here: https://github.com/athieffry/T1International-OoPE-survey-2022.
Ethics statement
The requirement of ethical approval for the studies involving humans was waived by the Human Research Ethics Committee – Humanities (HREC-HS) of the University College Dublin (HS-E-22-33-ODonnell). The study was conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
Author contributions
KS: Formal analysis, Investigation, Project administration, Resources, Writing – original draft, Writing – review & editing, Methodology, Supervision. EP: Conceptualization, Investigation, Writing – original draft, Writing – review & editing, Resources, Project administration, Supervision. AT: Data curation, Formal analysis, Methodology, Visualization, Writing – original draft, Writing – review & editing. YC: Formal analysis, Methodology, Resources, Writing – original draft, Writing – review & editing. KB: Resources, Writing – original draft, Writing – review & editing. MKB: Writing – original draft, Writing – review & editing, Resources. RS: Resources, Writing – original draft, Writing – review & editing. PG: Resources, Writing – original draft, Writing – review & editing. SO: Supervision, Writing – review & editing, Project administration, Writing – original draft.
Funding
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. This independent work was supported by funding from T1International with no third party involved. The use of REDCap was supported by the Center for Clinical and Translational Science and Training grant UL1TR001425 at Cincinnati Children’s Hospital Medical Center.
Acknowledgments
We would like to thank the members and alumni of T1International’s Global Advocacy Network who helped promote the 2022 OoPEs survey in their countries and communities. We are grateful to the eight pilot testers who reviewed the survey and provided their insight and feedback. Additionally, we are grateful to Sharon Sauter, Christina Barklund, and Faith Amasowomwan for their valuable review of the manuscript. Finally, we would like to thank the survey participants who shared their experiences.
Conflict of interest
EP is employed as the Executive Director of T1International. KS had a contract with T1International as the Global Advocacy Consultant. AT contracted with T1International to carry out quantitative analyses.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found here:
